Before Starting a Statin
Ask: Is it your lifestyle, genetics, or is your body internally overproducing risk?
1. Select your current age group:
2. Do you currently smoke or lead a primarily sedentary (little/no exercise) lifestyle?
3. Is there a family history of high cholesterol or early heart events?
The Vascular Multi-Hit Theory
Heart disease is rarely caused by a single factor. It is a "multi-hit" process where your Genetics meets External Stressors (Smoking, Inactivity, and High Blood Pressure).
Lifestyle vs. DNA: The "TOFI" Risk
Many high-functioning professionals are "Thin-on-the-outside, Fat-on-the-inside" (TOFI). You can be physically active and still have high cholesterol if your liver is genetically programmed to overproduce LDL. Conversely, smoking acts like "sandpaper" on your arteries, making it easier for cholesterol to seep in and form plaque.
Age-Specific Risk Audit
20–39: Start Line
Exposure matters during this stage. Cumulative LDL over 20 years creates a "base layer" of damage that is often invisible until later.
40–59: Red Zone
Metabolic resilience that used to buffer risk now begins to fail. This is the era where Soft Plaque begins to accelerate.
60+: Preservation
Focus shifts to protecting vascular elasticity and preventing sudden events that lead to hospital stays and loss of independence.
The Anatomy of a Heart Attack: Understanding Your Risk Era
Many patients ask: "If my cholesterol is only slightly high, why do I need a statin?" The answer isn't just about the blood test. It's about Plaque Stability.
The Biological Pivot
- 🔴 Before Treatment (The "Pimple"): High-risk plaque is soft, liquid, and fatty. Like a pimple with a thin skin, it is prone to "popping" (rupturing) under stress or high blood pressure.
- 🟢 After Treatment (The "Scar"): Statins help pull the liquid cholesterol out of the artery wall. The body then replaces that space with calcium, turning the soft "pimple" into a tough, stable "Vascular Scar."
The Result: A scar is structurally sound. It won't 'pop'. This process is known as Preservation. It's what actually prevents heart attacks, regardless of your LDL number.
This is why we focus so heavily on the Red Zone (Ages 40–59). During these high-stress professional years, we want to ensure your vascular infrastructure is "rupture-proof."
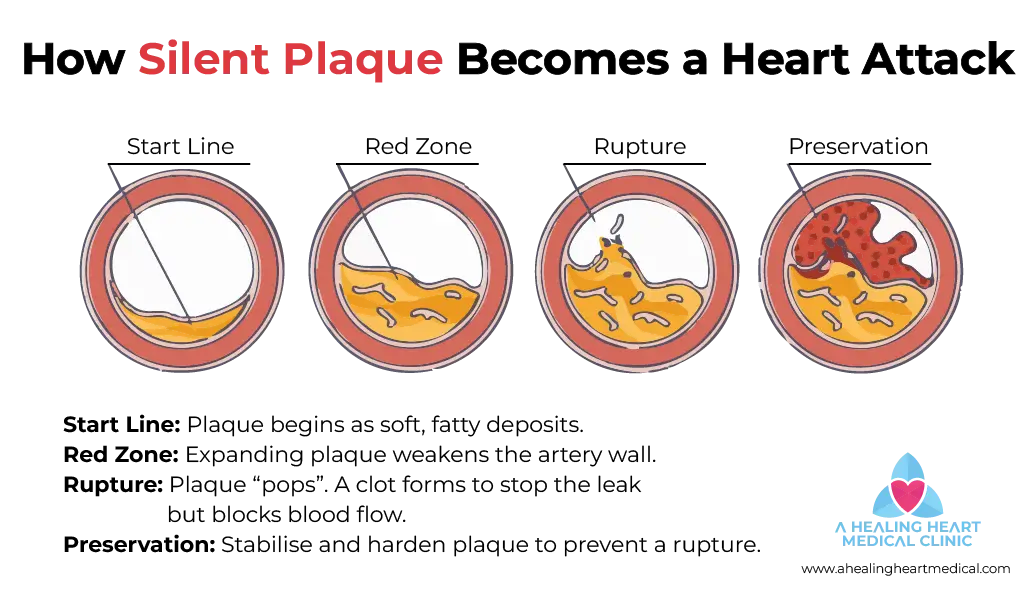
Figure 1: It shows the Vascular Timeline in a cross-section of an artery. From the Start Line where plaque is soft and reversible, to the Red Zone where it becomes unstable, our goal is to achieve Preservation by stabilizing and hardening the plaque to prevent a sudden rupture.
Clinical Side-Effect Audit
In a clinical audit, we weigh the minimal risk of medication against the significant risk of a "silent" vascular event. These figures represent documented cases in large-scale clinical populations.
| Your Concern | Clinical Reality | What this means for you |
|---|---|---|
| Muscle Pain (Myalgia) | < 5% | True statin-induced muscle damage is rare. 95% of patients experience zero muscle interference. |
| Liver Enzyme Elevation | < 1% | Effect is 1 in 100. It is usually a transient "stress" on the liver that reverses fully if the dose is adjusted. |
| New-Onset Diabetes | ~0.1% | This is 1 in 1000. It typically only occurs in patients who were already "borderline" or pre-diabetic. |
Your Pre-Consult Homework
To make your "Vascular Audit" more efficient, please have the following ready:
- ✅ Genetic Baseline: Identify any immediate family members (parents/siblings) who had heart events or strokes before age 55.
- ✅ Supplement Audit: List any natural cholesterol "remedies" you use, specifically Red Yeast Rice, CoQ10, or high-dose Fish Oil.
- ✅ Medication Audit: Note the name and dosage of any statins you are currently taking or have tried in the past.
- ✅ Muscle Baseline: Differentiate between general "gym soreness" and persistent, unexplained muscle heaviness.
The Long-Term Vision
A statin is a clinical tool to help you prevent future events. It is not a "life sentence." Its primary job is Vascular Insurance. Just as you wouldn't remove a 'seat belt' while driving at high speeds, we don't pause therapy suddenly while your risk factors are high or have just stablised.
What is a Metabolic Pivot?
If a patient achieves a true Metabolic Pivot (e.g. documented weight loss, a consistent shift in insulin sensitivity, and structural improvement in their vascular audit), we can then discuss a supervised reduction or "statin holiday." Our goal is the lowest effective dose required to keep your arteries stable.
Vascular Audit: Frequently Asked Questions
Why does Dr. Gerald Thang call ages 40–59 the "Red Zone"?
In Singapore, metabolic resilience typically begins to decline after 40. This is when silent vascular erosion accelerates. The goal isn't just a lower number on a lab report. The goal is Structural Integrity. We want to make sure our patient's arteries are less likely to rupture while they are at the peak of their careers and stress levels.
Is it possible to have high cholesterol if I am thin and active?
Yes. This is the 'TOFI' (Thin-Outside-Fat-Inside) profile. It is often driven by genetics, where your liver overproduces LDL regardless of exercise. For these patients, lifestyle changes have a ceiling (limitation), and clinical intervention is required to protect the arterial lining.
Will statins cause permanent liver or muscle damage?
No. Clinical reality shows that liver enzyme elevations (Less than 1%) and muscle aches (Less than 5%) are almost always reversible upon stopping or switching the medication. Regular blood audits are usually done to ensure total safety during treatment.
Can I take Red Yeast Rice instead of a statin?
Red Yeast Rice contains monacolin K, which is chemically similar to certain statins but without the standardized dosage or clinical safety monitoring. During your audit, we discuss if a pharmaceutical-grade medication and doctor-led monitored approach is safer for your specific risk profile.